
by Robert Nelson, MD, publisher Forum for Healthcare Freedom
Misinformation #2: Vaccine immunity is superior to COVID natural immunity.
The CDC accurately lists natural immunity as one of two ways to achieve protection from infection; the second way being vaccination against a specific pathogen. These two methods are referred to as “active immunity” or “acquired immunity.” To quote from the CDC website:
Either way, if an immune person comes into contact with that disease in the future, their immune system will recognize it and immediately produce the antibodies needed to fight it. Active immunity is long-lasting, and sometimes life-long.
 But here is an important caveat; not all viruses are created equal regarding their effect on the immune system. This is particularly true of respiratory RNA viruses such as RSV, Rhinovirus and seasonal Coronaviruses. These viruses have a knack for evading or blunting our immune response resulting in incomplete protection. Once we recover, sometimes these viruses can re-infect us. As a rule, most of these re-infections are mild given that our immune systems recognize and react to the infection more effectively with subsequent exposures.
But here is an important caveat; not all viruses are created equal regarding their effect on the immune system. This is particularly true of respiratory RNA viruses such as RSV, Rhinovirus and seasonal Coronaviruses. These viruses have a knack for evading or blunting our immune response resulting in incomplete protection. Once we recover, sometimes these viruses can re-infect us. As a rule, most of these re-infections are mild given that our immune systems recognize and react to the infection more effectively with subsequent exposures.
This process of viral innate immune evasion is, in large part, the back-story behind the oft repeated saying, “there’s no cure for the common cold.” This immune evasion is also why vaccine development for these ubiquitous infections has been challenging, to say the least.
When it comes to RNA respiratory viruses like COVID and others, it’s safe to conclude that neither natural immunity nor vaccine-induced immunity are 100% effective at preventing subsequent infections. Thus, we should prepare to co-exist with SARS-CoV-2 for a long time.
But how effective is natural immunity compared to vaccine-induced immunity at preventing subsequent infection, especially severe infections requiring hospitalization? The data looks pretty good in favor of natural immunity, especially in terms of durability.
Jeffrey Klausner, MD, MPH, and Noah Kojima, MD discuss this issue in their Op-Ed: Quit Ignoring Natural COVID Immunity | MedPage Today
“The range of reduction of re-infection from COVID-19 was between 82% to 95% among six studies that encompassed nearly 1 million people conducted in the U.S., the U.K., Denmark, Austria, Qatar, and among U.S. Marines.
The study in Austria also found that the frequency of re-infection from COVID-19 caused hospitalization in only five out of 14,840 (0.03%) people and death in one out of 14,840 (0.01%).
Raw data analysis from a large cohort study comparing natural immunity to vaccine-induced immunity showed the rate of subsequent COVID infections in natural recoverees to be 19 out of 16,215 for a rate of 0.12% compared to a rate of subsequent infections in virus-naïve vaccine recipients of 1.5%. While both offer good protection, the differential is nearly 13-fold in favor of natural immunity.
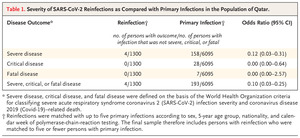 Another recent study published in the New England Journal of Medicine based on the Qatar national database of all SARS-CoV-2 primary infections from February 28, 2020 to April 28, 2021 looked at the risk of severe, critical and fatal COVID disease caused by reinfection. The rate of reinfection during the study period was only 0.5% (1,304 out of 265,779). Maybe more importantly, the odds ratio of severe re-infection compared to primary infection was 0.12 and there were ZERO critical re-infections and ZERO deaths in the other 1,300 cases.
Another recent study published in the New England Journal of Medicine based on the Qatar national database of all SARS-CoV-2 primary infections from February 28, 2020 to April 28, 2021 looked at the risk of severe, critical and fatal COVID disease caused by reinfection. The rate of reinfection during the study period was only 0.5% (1,304 out of 265,779). Maybe more importantly, the odds ratio of severe re-infection compared to primary infection was 0.12 and there were ZERO critical re-infections and ZERO deaths in the other 1,300 cases.
Given what we know about the ability of natural immunity to protect against many infectious diseases, including COVID-19, the CDC’s silence on the benefits of natural immunity has been puzzling, to say the least.
The latest attempt by CDC to claim superiority of vaccine-induced immunity over natural immunity is based on a study in their own MMRW released in October 2021. This was an oddly designed study if the goal was to compare vaccine-induced immunity to immunity generated from natural infection and the likelihood of subsequent COVID infection between the two groups.
An analysis by Martin Kulldorff shows that it was designed to answer whether hospitalized patient with COVID-like symptoms were more likely due to COVID or something else. The results indicate that the control group (COVID symptoms with something other than COVID) were more likely to have other serious respiratory illnesses such as pneumonia and tended to be older and frail. And therefore, they were not representative of the same population as the positive cases because they were more likely to be vaccinated due to being older.
If the authors wanted a valid comparison between the two groups, a preferred design would have been to compare cohorts such that the two properly matched and controlled groups could be reliably compared against the outcome of COVID infection (Reinfection vs breakthrough); as was done in the large Israel cohort study with over 16,000 participants in each group which were matched for age, gender, geographic region and other factors, making them comparable.
There are several other weaknesses of the CDC MMWR study. First, no serologic studies were done on the vaccinated group to see if they potentially had mild or asymptomatic COVID infection prior to vaccination. Several epidemiologic studies early in the pandemic estimated asymptomatic cases could account for about 15 – 20% of all infections. Although it’s impossible to estimate how many of the vaccinated group may have had undetected COVID infection prior to vaccination, it’s hard to believe that it was zero.
We also know the proportion of vaccinated persons hospitalized with COVID-like symptoms in the study outnumbered the unvaccinated by a ratio of nearly 6:1, despite the fact that only about 41% of the eligible population was fully vaccinated at the mid-point of the study indicating non-representative samples. Also, 16% of the hospitalizations in the non-vaccinated occurred between January and March whereas zero vaccinated individuals were hospitalized during that time frame.
The bottom line is, based on the data we don’t know the proportions of the general population, broken down by vaccinated and non-vaccinated status, who were at-risk for hospitalization. Drawing firm conclusions becomes impossible when cases and internal controls are not representative of the populations from which they are extracted.
These findings are in contradistinction to the Israeli study of well-matched and controlled cohort groups of equal size which showed a 13-fold increased chance of subsequent infections in the virus-naïve vaccinated cohort compared to the unvaccinated recoverees when the infection or vaccination occurred in January or February 2021. Allowing for infection to occur anytime between March 2020 and December 2020, there was a nearly 6-fold increased chance of subsequent COVID infection in the vaccinated virus-naïve cohort compared to unvaccinated recoverees. There was also an approximately 7-fold increase likelihood of COVID infections requiring hospitalization in the vaccinated cohort compared to the unvaccinated recoverees.
When two different studies that allege to look at the same issue or ask the same question, yet come to different conclusions, they both can’t be true. The preponderance of the evidence from dozens of studies supports the conclusion that naturally acquired COVID immunity substantially lowers the rate of repeat infections compared to vaccination only, has better durability compared to vaccine-induced immunity and markedly lowers risk of critical illness and death associated with reinfections.
It’s time to elevate natural immunity to the credible status that it deserves. The evidence demands it.
